High-pressure balloon dilatation in children: our results in 30 patients with POM and the implications of the cystoscopic evaluation
HTML: 32
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
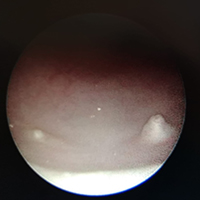
Primary Obstructive Megaureter (POM) is a common cause of hydronephrosis in children with spontaneous resolution in most cases. High-Pressure Balloon Dilatation (HPBD) has been proposed as a minimally invasive procedure for POM correction in selected patients. The aim of the paper is to review our experience with HPBD in patients with POM. We performed a retrospective study in a single Centre collecting data on patients’ demographics, diagnostic modalities, surgical details, results and follow-up. In particular, the endoscopic aspect of the orifice permitted the identification of 3 patterns: adynamic ureteral segment, stenotic ureteric ring and pseudoureterocelic orifice. We performed HPBD in 30 patients over 6 years. We had 23 patients with adynamic distal ureteral segment (type 1), 4 with stenotic ring (type 2) and 3 with ureterocelic orifice (type 3). In 3 patients (10%) the guidewire did not easily pass into the ureter requiring ureteral stenting or papillotomy. Post-operative course was uneventful. Five patients (3 pseudoureterocelic) required open surgery during follow-up. HPBD for the treatment of POM is a safe and feasible procedure and it can be a definitive treatment of POM. Complications are mainly due to double J stent and none of our patients had symptoms related to vescico-ureteral reflux. The aspect of the orifice, identified during cystoscopy, seems to correlate with the efficacy of the dilatation: type 1 and 2 are associated with good and excellent results respectively; type 3 do not permit dilatation in almost all cases requiring papillotomy. HPBD can be performed in selected patients of all paediatric ages as first therapeutic line. The presence of a pseudoureterocelic orifice or long stenosis might interfere with the ureteral stenting and seems associated with worse outcomes.
Altmetrics
Downloads
Citations




How to Cite
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
Similar Articles
- George Vlad Isac, Gabriela Mariana Danila, Sebastian Nicolae Ionescu, Spontaneous resolution and the role of endoscopic surgery in the treatment of primary obstructive megaureter: a review of the literature , La Pediatria Medica e Chirurgica: Vol. 45 No. 2 (2023)
- Salvatore Fabio Chiarenza, Cosimo Bleve, Elisa Zolpi, Francesco Battaglino, Lorella Fasoli, Valeria Bucci, Endoscopic balloon dilatation of primary obstructive megaureter: method standardization and predictive prognostic factors , La Pediatria Medica e Chirurgica: Vol. 41 No. 2 (2019)
- Antonio Marte, Staghorn stone in megapolycalicosis in a child: Still the case for open surgery? Case report , La Pediatria Medica e Chirurgica: Vol. 44 No. 1 (2022)
- Chiara Costantini, Federica Fati, Elisa Pani, Fabio Beretta, Silvia Bisoffi, Giosuè Mazzero, Elisa Negri, Clara Revetria, Hamid R. Sadri, Enrico Ciardini, Two-balloon epistaxis catheter to ensure vaginal patency in a complex case of vaginoplasty for vaginal agenesis: a case report , La Pediatria Medica e Chirurgica: Vol. 45 No. 2 (2023)
- Alessandro Calisti, Kibreab Belay, Andrea Mombo, Faisal Abdelgalil Nugud, Diaaeldinn Yaseen Salman, Pierluigi Lelli Chiesa, Presentations of bladder exstrophy in a resource-limited setting and the role of Mainz II continent diversion for late referrals or failed primary closures: a multicentric report , La Pediatria Medica e Chirurgica: Vol. 45 No. 2 (2023)
- Salvatore Fabio Chiarenza, Elena Carretto, Valeria Bucci, Samuele Ave, Giuseppe Pulin, Cosimo Bleve, Uretero-pelvic junction obstruction in children: Is vascular hitch an effective and safe solutions in very long term outcome? Report of 25 years follow-up , La Pediatria Medica e Chirurgica: Vol. 45 No. 1 (2023)
- Salvatore Arena, Tiziana Russo, Patrizia Perrone, Carmelo Romeo, Operative cystoscopy in the neonatal period , La Pediatria Medica e Chirurgica: Vol. 38 No. 3 (2016)
- Alessandro Calisti, Diaaeldinn Yaseen Salman, Kibreab Belay, Andrea Mombo, Boniphace Tresphory, Giovanni Giuliani, Martina Sertori, Gian Battista Parigi, The hidden burden of Pediatric urology in Sub-Saharan Africa: an analysis of hospital admission data from three East African Health Centres , La Pediatria Medica e Chirurgica: Vol. 46 No. 1 (2024)
- Carmine Noviello, Mercedes Romano, Letizia Trotta, Giuseppina Rosaria Umano, Alfonso Papparella, Are the complications after laparo-assisted endo-rectal pull-through for Hirschsprung disease related to the change of the anal tone? , La Pediatria Medica e Chirurgica: Vol. 46 No. 1 (2024)
- Leone Giordano, Salvatore Toma, Francesca Palonta, Roberto Teggi, Marco Zucconi, Stefania Di Candia, Mario Bussi, Obstructive sleep apnea in Prader-Willi syndrome: risks and advantages of adenotonsillectomy , La Pediatria Medica e Chirurgica: Vol. 37 No. 2 (2015)
You may also start an advanced similarity search for this article.


